| Disease name and synonyms Fungus ball of the sinus (saprophytic fungal sinusitis, aspergilloma of the sinus) |
| Fungi responsible Usually Aspergillus fumigatus, sometimes other species of Aspergillus, rarely other filamentous fungi. |
| Disease description Sinus aspergilloma develop in areas of functional or anatomical abnormalities; root-filling material has also been implicated in the pathogenesis. Chronic sinus symptoms such as purulent nasal discharge, obstruction, facial fullness, and facial discomfort are typical but non-specific. Post-nasal discharge and chronic cough is an occasional presentation. About 10% of patients are asymptomatic. The mean age at diagnosis is over 40 years, but all ages beyond teenager years can be affected. Unilateral sinus involvement is typical with the maxillary sinus most frequently affected. In 10% of cases the sphenoid sinus is involved. The fungal mass is clearly demarcated from normal sinus tissue with no evidence of invasion of tissue. There may be thickening or sclerosis of the sinus wall possibly attributable to pressure and pressure necrosis may ensue. The aspergilloma is a cheesy, friable brown, tan, green, yellow or black material. The fungal ball consists of a dense conglomerate of hyphae arranged in concentric circles |
| Frequency and global burden Fungus ball of the sinus has a global distribution. In a large study of endoscopic sinus surgery from Brazil, 33 of 890 (3.7%) had a fungal ball. In a large French university hospital, 13 cases were seen annually each year. Maxillary sinuses are affected in 85% of cases. |
| Underlying problems and at risk patients The vast majority of patients are not immunocompromised, but data suggests that diabetes, hypertension and haematological disorders are more frequent. Patients are not more often atopic than the general population. Women are more frequently affected. There are some anatomical variations in the nose and sinuses that are more common in those with fungal ball of the maxillary sinus: Prior dental work on the upper molars and second premolar teeth, presence of a concha bullosa which tends to be larger (which alters air flow through the nose), less frequent presence of Haller cells and a wide maxillary sinus ostium. Patients are not more often atopic than the general population. |
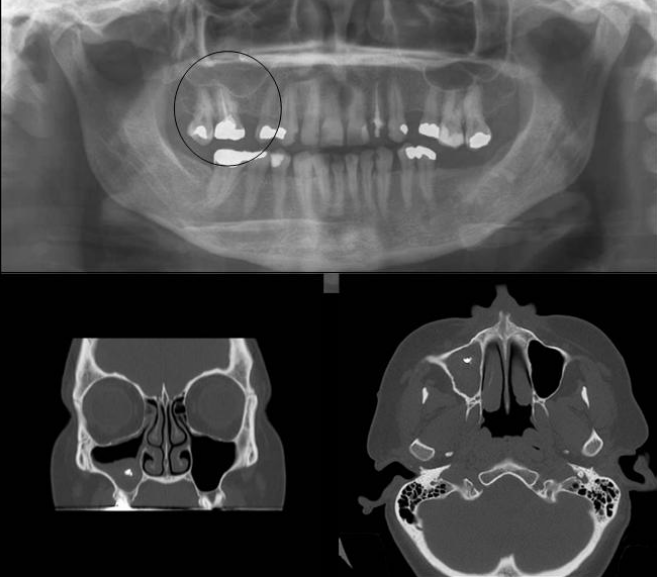
| Diagnostic testing CT scans usually show sinus opacification, with or without discrete calcification or metallic densities surrounded by spiculated or linear areas of microcalcification. Sometimes a pseudotumor appearance is seen. Thickening of the walls of the involved sinus may be seen as may bone erosion or remodeling. Histologically, the sinus mucosa is well preserved other than a chronic non-granulomatous inflammatory response which may be a pressure effect. Direct smears are usually positive for hyaline septate hyphae. Cultures are often negative (~70%) and A. fumigatus is the most frequently grown fungus. S. apiospermum may occasionally be cultured as may other Aspergilli. Galactomannan is usually detectable. |
| Treatments Endoscopic endonasal surgery is the definitive treatment of choice. The precise technique depends on localisation (ie middle antrostomy, sphenoidotomy, ethmoidectomy). It is appropriate to treat asymptomatic patients if there are no additional risks. Biopsies of the mucosa are not required (ie to document an absence of invasion), if the fungal ball comes away cleanly from the sinus wall. Antifungal treatment is not required. |
| Outlook and prognosis Excellent outlook, with almost no relapse, if all the material is removed and sinus drainage improved. |