| Disease name and synonyms Granulomatous invasive fungal rhinosinusitis (chronic granulomatous fungal rhinosinusitis or primary paranasal Aspergillus granuloma) |
| Fungi responsible Aspergillus flavus is the commonest agent isolated. Other Aspergillus species like A. fumigatus and A. niger have been isolated. Rarely black mycelial fungi like Bipolaris spp. and hyaline fungi like Schizophyllum commune have been isolated. |
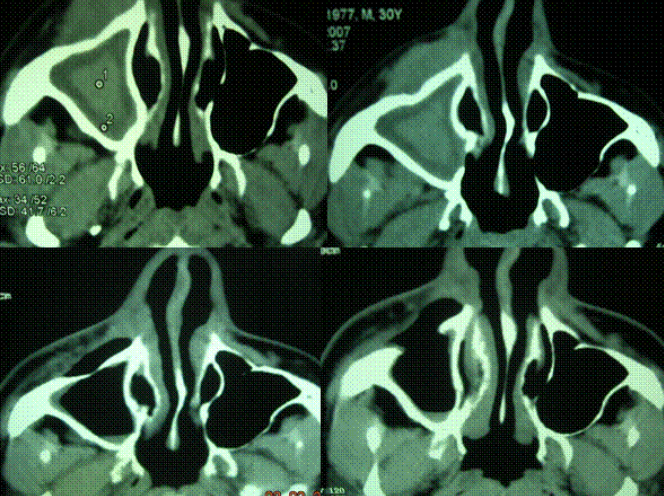
| Disease description Patients usually come to clinical attention with nasal obstruction, enlarging mass in the cheek, orbit, nose, maxillae, and paranasal sinuses. Sometimes proptosis or cranial nerve palsies are the reason for medical attention. The disease has a gradual onset and takes a chronic course, usually over many months, and sometimes years. The patients are typically immunocompetent. CT imaging reveals a soft tissue mass in one or more paranasal sinuses, usually with extension to orbit or brain. Chronic granulomatous fungal sinusitis appears endoscopically as a firm to hard mass in the nasal cavity which often extends to the adjoining sinuses (ethmoids or maxillary sinus) and to the orbit, especially if proptosis present. The mass is relatively avascular and often does not bleed on biopsy |
| Frequency and global burden Up to 30% of cases of chronic fungal rhinosinusitis are in fact granulomatous invasive fungal rhinosinusitis in certain geographic location including Sudan, middle east and India. In USA and Europe the disease is rare, though in some series cases up to 2% of all chronic fungal rhinosinusitis have been reported as invasive. |
| Underlying problems and at risk patients The disease occurs in apparently healthy hosts. The disease is prevalent (~70%) in inhabitants of tropical regions, especially those active in farm work. |
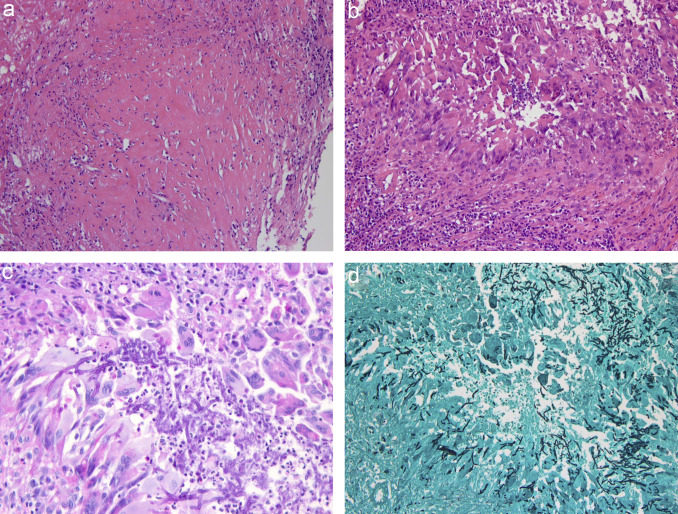
| Diagnostic testing The disease is often initially mistaken for malignancy based on nasal endoscopy and CT imaging as it has a mass-like appearance. The diagnosis is made on histopathology of the biopsy taken or mass removed during surgery. Histopathologically, a granulomatous response is seen with considerable fibrosis. Non-caseating granuloma with foreign body or Langhan’s types of giant cells may be seen, sometimes with vasculitis, vascular proliferation and perivascular fibrosis. Occasionally central microgranulomata of eosinophils, fibrinoid necrosis are also seen. In contrast to the chronic invasive variety, hyphae are scanty and seen commonly inside the giant cells without any vascular invasion. A. flavus is primarily isolated from these cases, if tissue is submitted for culture, which ti should be. If no fungi are detected or isolated, molecular technique extraction of fungal DNA and ITS sequencing help in clinching the diagnosis. In situ hybridization or immunohistochemistry may also help in diagnosis, although these tests are not readily available. Detection of precipitating antibody to A. flavus helps in supporting the diagnosis. With successful treatment, precipitating antibody titres fall and may rise again with recurrence of the disease. |
| Treatments Surgical removal of the mass and antifungal therapy with itraconazole or voriconazole or amphotericin B helps in cure. Usually endoscopic surgery is not sufficiently radical for sure, although occasionally the disease is caught early following complete removal of disease endoscopically. Timely management is effective. Recurrence is rare after prolonged antifungal therapy, which should be for a minimum of six months, if possible. |
| Outlook and prognosis Nearly all patients survive with radical resection surgery and antifungal therapy, if the diagnosis is not made too late. Patients with intracranial or orbital extension may be fatal, but almost always lead to considerable morbidity. |