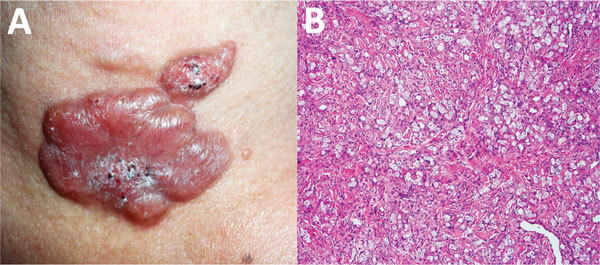
Lobomycosis (AKA lacaziosis) is an implantation mycosis endemic to the Amazon basin, caused by the uncultured fungus Lacazia loboi. It causes chronic subcutaneous disease with pleomorphic keloid-like lesions on the cooler areas of the body, particularly the lower limbs and ears. Progression is slow (years) and dissemination is rare, but the lesions can cause disfigurement.
Dr Claudia Arenas and colleagues in Bogota describe a series of 6 cases of lobomycosis in Colombian soldiers, acquired while they were stationed in the rainforest.
Direct smear for leishmaniasis amastigotes was positive in 3 (50%) of the cases, and in at least one case the Lacazia fungus was thought to have become implanted in a leishmaniasis lesion. Differential diagnosis can be challenging as lobomycosis has sometimes been found associated with lesions caused by concomitant infections (e.g. leprosy, leishmaniasis) or squamous cell carcinoma, and management of these factors can contribute to lesion healing.
- Lobomycosis can be diagnosed if microscopy (PAS/Grocott’s staining) of a skin biopsy reveals granulomatous inflammation without abscesses, and many phagocytised yeast cells that form chains
Antifungal drugs are not effective, so wide local excision is recommended. Lesions may recur many years after apparent cure.
- Read the paper: Arenas et al (2019)
- Read a review about lobomycosis: Francesconi et al (2014)
