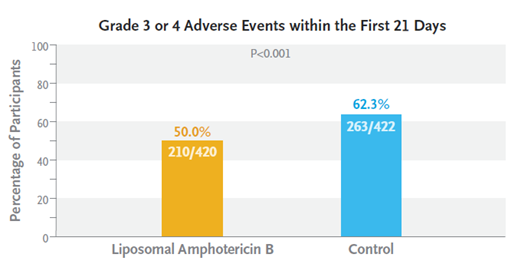
The world’s largest randomised study of HIV-positive adults with cryptococcal meningitis has shown that a single high-dose infusion of liposomal amphotericin B, plus oral therapy with flucytosine and fluconazole was non-inferior to standard treatment. This short course approach was also associated with fewer adverse events.
This research was carried out in 844 patients across five countries in sub-Saharan Africa, where cryptococcal meningitis is one of the main causes of death in people who are HIV-positive.
Traditional treatment using a one- or two-week amphotericin B deoxycholate-based regimen is superior to fluconazole monotherapy, which has poor outcomes in these patients. Even a one-week amphotericin B course increases risk of anaemia, kidney impairment, and electrolyte abnormalities, even if liposomal amphotericin B is used.
This new approach recommends a single high-dose intravenous infusion of liposomal amphotericin B (10mg/Kg), with oral flucytosine (100mg/Kg) and fluconazole (1200mg) given for 2 weeks. Professor Joe Jarvis and colleagues of the London School of Hygiene and Tropical Medicine showed this approach to be non-inferior to a one-week course of deoxycholate amphotericin given at 1mg/Kg daily.
The benefits of this new approach are shorter hospital stays, as only a single intravenous dose would need to be administered. This would make for a more cost-effective treatment.
The authors state: ‘The 10-week mortality of 24.8% observed in the liposomal amphotericin B group in our trial is among the lowest reported from a major cryptococcal meningitis trial in Africa, despite more than a quarter of participants presenting with very severe disease and abnormal baseline mental status. Our study results represent a notable improvement on the mortality rates of 40 to 45% reported in trials of 2-week amphotericin B deoxycholate–based regimens previously conducted in resource-limited settings.’
To find out more about the findings of this study click here.