Neglected tropical diseases (NTDs) are a diverse group of conditions caused by a variety of many parasites, a few bacteria (including leprosy) and fungi and toxins (especially snake bite) and are associated with devastating health, social and economic consequences. NTDs are mainly prevalent among impoverished communities in tropical areas, although some have a much larger geographical distribution. It is estimated that NTDs affect more than 1 billion people, while the number of people requiring NTD interventions (both preventive and curative) is 1.5 billion. The epidemiology of NTDs is complex and often related to environmental conditions. Many of them are vector-borne, have animal reservoirs and are associated with complex life cycles. All these factors make their public health control challenging.
The NTDs caused by fungi that are listed by the World Health Organization are deep skin infections – mycetoma, chromoblastomycosis and sporotrichosis. The G-Finder program also lists histoplasmosis. The journal PLoS NTDs includes paracoccidioidomycosis which has been informally adopted by the Pan-American Health Organisation as an NTD. The case for fungal keratitis to be listed as an NTD was not accepted by the WHO.
Find out what the World Health Organization are doing to combat NTDs here.
Chromoblastomycosis
| Disease name and synonyms Chromoblastomycosis For further information, there is a GAFFI factsheet on chromoblastomycosis. |
| Fungi responsible Can be caused by a number of different pigmented fungi, the most common of which are Fonsecaea pedrosoi, Fonsecaea monophora and Cladophialophora carrionii. Other fungi occasionally also cause chromoblastomycosis, such as Rhinocladiella aquaspersa and Rhinocladiella similis. |
| Disease description Chromoblastomycosis presents with wart-like lesions on exposed areas of the skin such as the legs or forearms. These can exceed 10 centimetres in diameter. Patches of skin may also appear flattened (plaque-like) and show central scarring or atrophy, but they are not itchy or painful. Pain and itching can appear in moderate or severe disease. Small dark spots can be seen on the surface of lesions and represent clusters of the pigmented fungal cells – an important diagnostic clue. Large lesions cause severe limb swelling and discomfort, limiting movement. In longstanding cases, secondary bacterial infections are common and the smell from affected limbs may be unpleasant, which may also lead to social exclusion. There is a risk of development of squamous cell carcinoma of the skin in longstanding untreated lesions. Although the infection usually remains in one body region, local spread through the lymphatics, and very rarely blood stream dissemination to the central nervous system, can occur. Chromoblastomycosis can cause disability due to limb enlargement, which may lead to inability to work and considerable social stigma. Rarely, the fungi that cause chromoblastomycosis can infect other organs, such as the brain, or lead to skin cancer. |
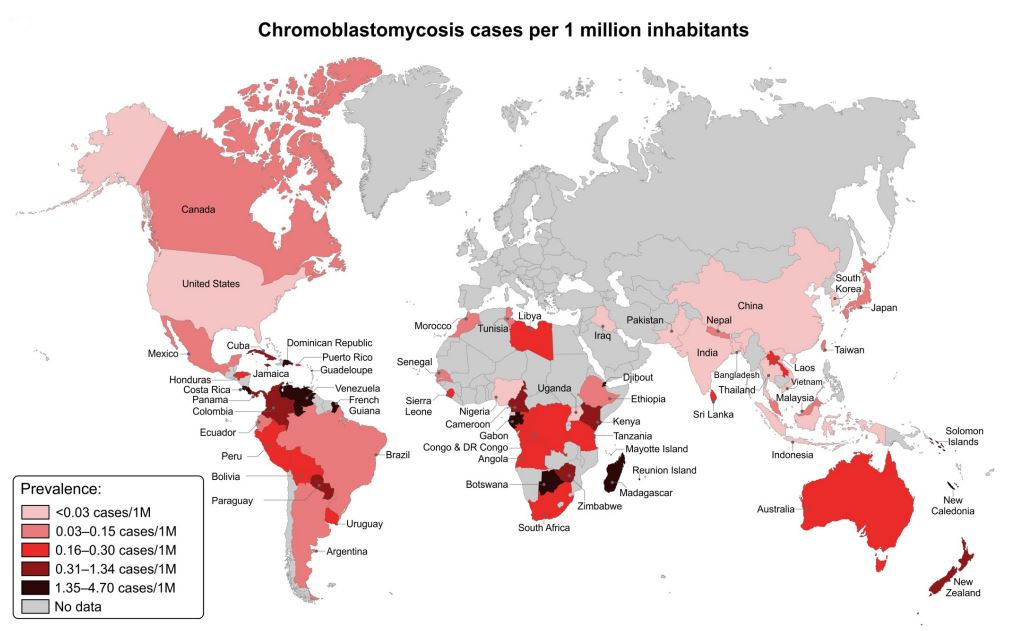
| Frequency and global burden The global incidence remains unclear and local epidemiological studies are required to improve the data especially in Africa, Asia, and Latin America Santos et al has provided a map of the incidence rate of CBM. |
| Underlying problems and at-risk patients The disease especially affects men (81.7% in Santos et al), with a mean age of 57 years. Lower and upper limbs are the most compromised sites, with verrucous, tumoral and plaque representing the main dermatological patterns. Chromoblastomycosis affects normal healthy people and is mainly seen in adults. Agricultural workers are the most common occupational group to be infected. One occupational group that are particularly affected are the babassu nut farmers in Brazil. |
| Diagnostic testing Culture or molecular diagnosis is helpful in confirming the diagnosis but decisions on treatment can be made without identification of the organism. Samples are taken from a skin biopsy or skin scraping. The characteristic histologic finding is the presence of muriform cells, which appear as chestnut to rounded brown pigmented and cross septated structures. All the causative fungi grow slowly in culture, with usually a deep green colour, becoming dark and velvety over time. |
| Treatment Chromoblastomycosis can be treated with oral itraconazole or terbinafine. Voriconazole, intravenous amphotericin B and oral flucytosine have also been used. Other methods of treatment include local application of heat, cryotherapy and photodynamic therapy. Surgical reductions have been used but should be given following initial chemotherapy to avoid local recurrence. |
| Outlook and prognosis Early treatment is key, providing the best results after about 3–6 months. Patients with large or extensive chromoblastomycosis and limb swelling often require over a year of treatment and there may be residual lymphoedema in such cases. |



Mycetoma
| Disease name and synonyms Mycetoma; eumycetoma when caused by fungi, actinomycetoma when caused by bacteria. For further information there is a GAFFI factsheet on mycetoma. |
| Fungi responsible The most common fungal causative agents are Madurella mycetomatis, Madurella tropicana, Madurella fahali and Scedosporium apiospermum. |
| Disease description The disease is characterised by a painless subcutaneous mass, multiple sinuses and purulent or seropurulent discharge containing mycetoma grains. Grains are of various colours, sizes and consistent with the causative organism. The subcutaneous mass usually spreads to involve the skin and deep structures, resulting in destruction, deformity and loss of function – occasionally it can be fatal. In more than 80% of patients mycetoma affects the hand or foot. Occasional cases of head and neck, chest, abdominal wall, perineum or gluteal region are recorded. Rare mycetoma sites include the eye, sinuses, mastoid bone and scrotum. Eumycetoma has a slower progression than the more rapidly invasive actinomycetoma, but ultimately can be just as destructive. |
| Frequency and global burden The disease is endemic in many tropical and subtropical regions across the world, with high prevalence in the ‘mycetoma belt’. The belt stretches between 150⁰S and 300⁰N, and includes Sudan, Somalia, Senegal, India, Yemen, Mexico, Venezuela, Columbia, Argentina, and Iran, amongst others. There are probably between 20,000 and 50,000 cases worldwide based on literature reports. Most cases are reported from Sudan, Mexico and India. |
| Underlying problems and at-risk patients The most common age of infection is young adulthood (70% of the cases are between ages 11 and 40), with some children and older people affected. In most countries men are affected more than women. |
| Diagnostic testing Surgical biopsy is important to obtain grains for culture, molecular identification and histopathological examination. Individual grains have a distinctive appearance under direct microscopy, depending on causative agent, but this is insufficient to determine the bacteria or fungi responsible for the infection. Culture requires a range of media, including fungal, bacterial and mycobacteria plates and/or liquid culture. Years of experience are required to identify all of the fungi and bacteria that cause mycetoma, and there are many variants and isolates that resemble others. It is recommended to plate as many grains as possible in order to increase the chance of culturing the organism. Formal genetic identification using sequencing is most reliable. Susceptibility testing is not standardized and has not been well correlated with treatment outcome. Various imaging modalities are useful to define the extent of disease. Conventional X-ray, ultrasound to identify grains and MRI all have an essential place in determining the disease spread, and to establish a disease management plan. Currently, the available diagnostic tests and techniques are invasive, tedious and expensive. Most of them do not exist in endemic regions, and patients need to travel far to establish the diagnosis. |
| Treatment The treatment of eumycetoma involves a combination of antifungal treatment (currently itraconazole 400mg/day) and surgical excision. Excision ranges in extent from wide local excision to repetitive debridement, and in severe cases, amputation. Surgery is indicated for cases resistant to medical therapy and when the lesion is localised. It may be life saving in advanced disease that is complicated by secondary bacterial infection, sepsis, massive bone involvement, and poor general condition. Some data indicate that voriconazole may be a better treatment for certain organisms, notably Medicopsis (Pyrenochaeta) romeroi. Eumycetoma treatment is prolonged with a low cure rate and high recurrence and dropout rates. |
| Outlook and prognosis Eumycetoma patients usually respond poorly to medical therapy. Improvement is slow and hard to evaluate, even after months of treatment. Many patients eventually fail to complete education or lose their jobs. For more information on the treatment of mycetoma in Sudan, visit The Mycetoma Research Centre’s website. For more information on actinomycetoma see Dermatology Advisor |