Fungal spores are a common trigger for asthma, and the fungal burden within the lungs can be significant. There is increasing evidence that treatment with antifungals may be beneficial for patients with severe asthma who are sensitised to fungi.
Videos
Factsheets
SAFS
| NAMES SAFS, severe asthma with fungal sensitisation |
| DISEASE Severe asthma as defined by the 2009 ATS/ERS guidelines or earlier BTS guidelines. In practice this means a low FEV1 or peak flow (usually persistently), high dose inhaled steroids and/or frequent courses of oral steroids. Watch a patient experience video about sensitivity to Alternaria |
| FUNGI Many, some alone, some collectively. Especially Aspergillus fumigatus, Penicillium chrysogenum, Cladosporium herbarum, Alternaria alternata, Candida albicans, Trichophyton spp. and probably others. |
| GLOBAL BURDEN Probably worldwide. Severe asthma affects 5-20% of those with asthma, depending on definition and denominator. Of these, 35-50% have SAFS, depending on how extensively they are tested. Six million of people with SAFS are a conservative estimate. |
| RISK FACTORS Asthma. No specific risk factors identified. Possibly genetic in part. |
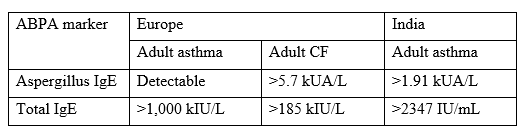
| DIAGNOSIS Total IgE may be normal or elevated, but is <1,000 KIU/L. Skin test or specific IgE test positive for any fungus. |
| TREATMENT Conventional treatment for asthma. Itraconazole (or another azole, but not fluconazole) benefits ~60% patients in terms of quality of life, although not necessarily improved lung function. CURRENT GUIDELINES |
| OUTLOOK Severe asthma is a debilitating disorder, with frequent medical contacts and multiple treatments. Poorly treated or late treatment results in some intensive care admissions or deaths each year, but it not known how many of these are in SAFS patients. |



Skin testing for fungal allergy
| INTRODUCTION In 1925, Van Leeuwen and colleagues described a remarkable frequency (50%) of mould skin sensitivity in Dutch asthmatics principally to Mucor, Penicillium and Aspergillus species. In 1928. Both Hansen in Germany and Jimenez-Diaz with colleagues reported positive skin tests to crude fungal extracts. The European Community Respiratory Health Survey showed that 36% of people with asthma had one or more positive skin prick tests, indicating that they were atopic. Of these, 4.4% were sensitised to Alternaria and 2.3% to Cladosporium, compared with 21% sensitised to house dust mite, 17% to grass pollen, and 10% to cat. There is also a high prevalence of fungal sensitisation among Africans with asthma. A review by Kwizera et al. reported a prevalence of fungal sensitisation of 3-52% in the asthmatic population, with an average of 28% and a pooled estimate of 23.3%, mostly due to Aspergillus species. The prevalence of allergic bronchopulmonary aspergillosis (ABPA) was estimated at 1.6-21.2%. Besides the allergens mentioned above, recent studies have emphasized occupational insect allergy and cannabis consumption as a risk for the development of asthma. |
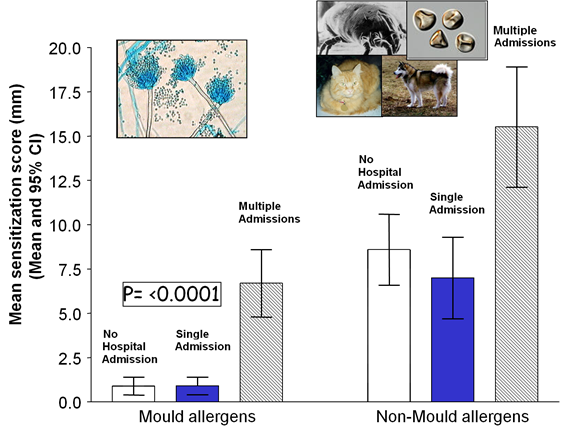
| LINK WITH SEVERE ASTHMA Fungal sensitisation is more prevalent in people with severe asthma and usually occurs following exposure to moulds. Detecting IgE specific to one or many fungi is a marker of severe asthma, sometimes referred to as brittle, difficult or poorly controlled asthma. The combination of severe asthma, fungal sensitisation and exclusion of ABPA and allergic bronchopulmonary mycosis (ABPM) is referred to as severe asthma with fungal sensitisation (SAFS). A review evaluating studies on fungal sensitisation associated with severe asthma identified ten fungal genera, of which sensitisation to Aspergillus, Penicillium, and Cladosporium species significantly increased the risk of severe asthma. Within the Aspergillus species, Aspergillus fumigatus-specific sensitisation demonstrated a stronger association with severe asthma. O’Driscoll et al., in a multicenter study, showed mould sensitisation may be linked with multiple hospital admissions in patients with severe asthma: 76% of patients with multiple admissions had at least one positive mould skin test compared with 16-19% of other asthma patients. Also, multiple mould reactions were much more common in the group with multiple admissions. |
| Robin Réau and colleagues, in a French prospective study, reported 28% of 254 adults with severe asthma had SAFS. This group had positive IgE assays to Aspergillus fumigatus (64%), and other fungi, including Alternaria, Candida, Penicillium, Cladosporium and Botrytis, with total IgEs <1000 IU/mL, but raised. A key finding from this study was the diagnosis of obstructive sleep apnoea in 25% of SAFS patients, compared with 9% in the severe asthmatics without SAFS. In addition, asthma exacerbation requiring hospital attendance or admission was documented in 36% of SAFS patients versus 19% in the non-SAFS asthma group. Also, the median predicted FEV1 was substantially lower in the SAFS group compared with the non-SAFS asthma group – 66% vs 77%. Despite the rising use of biologics (21% to 68%) in these patients, many of these parameters remained unchanged: the median FEV1 was still only 65% predicted in the SAFS group, 30% remained on oral corticosteroids, and 12% had attended or been admitted to hospital. |
| The management of SAFS includes adopting preventive strategies: removal of visible mould, no smoking indoors, opening the windows for at least 15 minutes daily to ventilate the bedroom and the living room and the removal of dust reservoir with a vacuum cleaner containing a HEPA filter are measures proven to reduce exposure to fungi if deployed. In addition, besides improving asthma, Gangneux and colleagues showed hospitalizations for asthma decreased from 28 to 4 over the 12-month intervention period, FEV1 increased by more than 12% for 60% of the intervention patients, and oral corticosteroid consumption fell by 71%. Dermatophytes like Trichophyton species have also been implicated in worse asthma due to their several potent IgE antigens. In addition, the treatment of skin fungal infection alleviates asthma, although the data demonstrating this is scanty. Thus, taking cognizance of this will also be a very useful preventive and or treatment strategy. Treatment should include the use of oral itraconazole, particularly as biologics seem only marginally effective. This is also economically favourable for those in poorer countries, as biologics are unaffordable in resource-poor settings. |
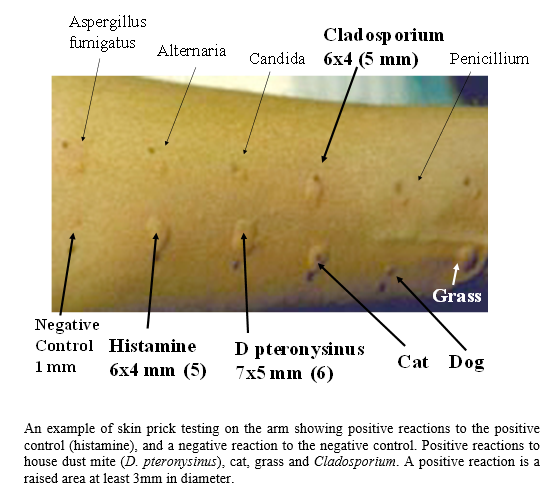
| ISSUES WITH SKIN TESTS Unfortunately, reagents from different manufacturers differ and give slightly different skin prick test results in different people. Skin test responses may vary over time in the same individual, even if performed in an identical manner with the same reagent. Asthma may also ‘go through good and bad periods’, possibly consistent with this. While the correlation between positive skin tests and IgE RAST test on blood is reasonable, there is enough discordance to require both to be done to identify all patients who are sensitized to fungi. Skin tests tend to be more sensitive. Some clinics test for a wide range of fungal sensitivity, others test for a limited number or only for Aspergillus fumigatus sensitivity. A reasonable minimum testing set is Aspergillus fumigatus, Candida albicans, Cladosporium herbarum, Alternaria alternata, Penicillium chrysogenum (notatum) and Trichophyton mentagrophytes. |
| IgE testing Fungal allergy is partly mediated through IgE binding to mast cells, leading to the release of histamine, which is recognized as an immediate-type hypersensitivity reaction. Delayed-type hypersensitivity is not mediated through IgE, but eosinophils and possibly basophils appear to be important mediators of inflammation. IgE can be directed at a specific fungus, and/or the total IgE can be elevated. A key diagnostic criterion of ABPA is an elevated total serum IgE. Different cut-off levels have been identified or proposed for different conditions and may also vary by test manufacturer. Commercial assays for total IgE include ImmunoCAPTM, ImmunoCAP ISAAC 112, Allergy Line, EUROLINE, AllergyScreen, RIDA qLine Allergy, Polycheck Allergy, DELFIA, ALercheck, inc, IMMULITE 2000, AlaStat, ALEX-2, MosaiQ® AllergyPlex™, HYTEC 288, IgE inhalant allergy test, NOVEOS, OPTIGEN, Allergia ELISA, Allergy Advance Panel, Accuris B+ve Allergy Panel, BioIC, BioCLIA® Allergy, PROTIA Allergy-Q, Human IgE(Immunoglobulin E) ELISA Kit (E-EL-H6104), AdvanSure, CLA ALLERGEN-SPECIFIC IGE ASSAY-LATEX ALLERGEN (K82), Spec. IgE S, amongst others. Cross-validation and comparative assays are not done for many of these assays. |
| A detectable Aspergillus-specific IgE is another key diagnostic criterion for ABPA (and allergic Aspergillus sinusitis) and defines Aspergillus sensitization, which is associated with reduced lung function in cystic fibrosis, chronic obstructive pulmonary disease and following pulmonary tuberculosis. Immediate skin prick tests against Aspergillus also detect Aspergillus IgE, but there is imperfect concordance between serum detection of Aspergillus IgE and skin testing. |
| Many different fungi and other allergens can induce sensitization. Fungal sensitization in childhood (especially Alternaria) is associated with persistent asthma later in life. Elevated fungal-specific IgE is one of the diagnostic criteria for SAFS and may be elevated in fungal rhinosinusitis. Fungal-specific serum assays are available from Thermo-Fisher and Siemens. Skin prick testing for fungal-specific immediate hypersensitivity (or IgE) also defines fungal sensitization. |
Thunderstorm asthma
Packe and Ayres (1985) first noted the association of thunderstorms with increased acute asthmatic attacks. At the time of the thunderstorm they found increase in airborne spores of the fungi Didymella exitialis and Sporobolomyces spp. Since then many episodes of thunderstorm asthma have been noted from different places.
Increased humidity and high winds triggers both increased fungal spore production and dissemination. Rapid increases of numerous other fungi in air, such as Alternaria spp. or grass pollens or both have been associated with thunderstorms and fungal spores may be more highly associated with asthma then pollen. Thunderstorm asthma was positively correlated with a doubling of ambient fungal spores.
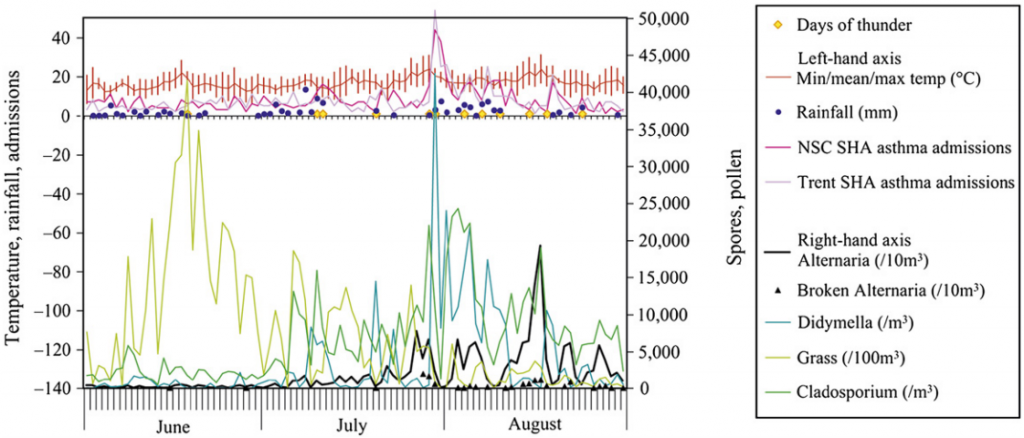
In North America, the central prairies of wheat fields generate huge quantities of Alternaria spores. In 1937, a ‘spore storm’ occurred throughout the eastern United States. Huge air masses travelled rapidly to the Atlantic seaboard, conveying several tons of fungal spores hundreds of miles. In London, an outbreak of asthma related to a thunderstorm was seen in 1994 (Celenza et al, 1986). The figure shows the spike in cases and they measured pollen counts, but took no fungal measurements.
Courtesy of Crown Preservation